As part of its BSafe campaign, the Britannia P&I Club describes a fatality of an electrician from electrocution, while performing maintenance of the inert gas scrubber electrical system, onboard an oil tanker. The electrician had been working alone at the time.
AS TYPICALLY OCCURS IN MANY SIMILAR INCIDENTS, THIS FATALITY APPEARS TO BE A RESULT OF A COLLECTIVE FAILURE OF A NUMBER OF SAFETY PROCESSES AND BARRIERS, WHICH SHOULD HAVE BEEN FULLY IMPLEMENTED AND MONITORED AS PART OF THE SAFETY MANAGEMENT SYSTEM (SMS).
The tragic death of the electrician could have been prevented if the safe work practices were adhered to. The apparent lack of challenge on multiple occasions points to an ineffective onboard safety culture, where unsafe acts were being tolerated and unsafe behaviours not stopped.
It is worth pointing out that the electrician had served in that capacity for 32 years, so a lack of experience was not a factor. As concluded by the investigation report, it is likely that he did not perceive the work as high risk due to its routine nature.
The case study and investigation identified a number of factors and lessons learned, as discussed below.
SAFE WORK PRACTICES
Although the Company’s SMS required completing a number of procedures (a formal risk assessment, a Permit to Work (PTW), Lock Out/Tag Out (LOTO) procedures and a Toolbox Talk) prior to the work being undertaken, none of these processes had been completed before work began. The investigation report did not identify any issues with the SMS or these procedures. As discussed further below, completion of each of these processes by the relevant crew members should have acted as safety barriers to prevent this incident.
The electrician was not questioned about the previously unplanned work during the morning planning meeting, or when he spoke with the engine cadet shortly before the incident.
CLEAR COMMUNICATION
The investigation identified a lack of clear communication between the second engineer (2/E) and the electrician regarding the maintenance of the starter panel as one of the causal factors that contributed to the fatal electrocution of the electrician. No information is available whether the language or cultural background were a factor.
The ability to communicate clearly and effectively is the key to the successful and safe operation of any ship. It has been recognised as a critical soft skill by its inclusion in specific requirements regarding effective communication in officer training in the 2010 Manila Amendments to the International Convention on Standards of Training, Certification and Watchkeeping for Seafarers (STCW).
In addition to any formal training, effective communication is a skill that needs to be practised daily. Safety-critical information should be acknowledged, understood and clarified if necessary. Ambiguity leads to making assumptions and may have a significant impact on safety.
RISK ASSESSMENT
It is unclear from the incident investigation to what extent there was a history of similar work being undertaken without the required, formal risk assessment.
On the day of the incident, when the electrician mentioned his plan to work on the inert gas (IG) scrubber pump starter panel, there was no reaction to the absence of a prior risk assessment during the morning meeting in the presence of the 2/E and the team.
If such lapses had occurred before and were not immediately rectified, it could have created a level of acceptance which in turn resulted in the lack of an appropriate challenge when due.
The investigation did note that a risk assessment was conducted and PTW had been prepared before maintenance was reportedly completed on the IG scrubber pump starter panel six days before the incident. This therefore suggests that the
2/E and electrician were apparently aware of the SMS requirements for these processes. However, this maintenance task was scheduled for completion every three months and it was also identified that the star contactor may have not been overhauled six days earlier as it should have been, according to the maintenance records; the investigation was not able to determine the reasons for this anomaly.
PERMIT TO WORK (PTW)
As an essential procedure performed on many occasions, PTWs are usually well rehearsed and the type of work which triggers the need for a PTW is well known. In a work environment where the SMS is effectively implemented and supported by an adequate safety culture, an attempt to carry out work without a PTW (if required) would result not only in stopping the work from starting, but also in raising a near miss or observation/non-conformity report.
A completed PTW would have required another crew member to be present during the work on the electrical equipment. The presence of another person could have provided a further opportunity for the unsafe activity of accessing the lower section of the cabinet containing the energised 440V circuits to be challenged and stopped.
The investigation report does not provide information whether the SMS record was analysed for evidence of previous, similar occurrences and how they had been managed. Any evidence of previous incidences would indicate a possible contributing factor.
APPLICATION OF LOCK OUT/TAG OUT
Completing a PTW would have required a verification that the LOTO procedures, as a core requirement, were completed. This in turn would have resulted in removing the hazard by de-energizing circuits and equipment in and around the work area.
The appropriate implementation of LOTO would likely result in the process becoming the norm for most of the electrical maintenance in the engine room. The fact that the electrician commenced work despite the absence of LOTO may indicate a possibility that this behaviour had previously been normalised.
STOP WORK AUTHORITY (SWA)
The SWA policy adopted by the Company did not work as intended on this occasion. A number of team members had the opportunity (and obligation) to stop the electrician from undertaking the task, but did not act. This included the 2/E, as the supervisor, and all team members involved, as well as the electrician himself. The investigation did not appear to consider whether there was evidence of the SWA being used effectively before the incident.
Ideally, the appropriate use of the SWA should be encouraged and supported, and as a result the team members would be more likely to react to an unsafe condition or behaviour by invoking the SWA and preventing an incident from occurring.
TOOLBOX TALK, JOB HAZARD ANALYSIS (JHA) AND HAZARD IDENTIFICATION
Among other requirements which were not met before the incident, the Company’s SMS stipulated that a job-specific Toolbox Talk should occur after obtaining the PTW but before commencing work. The morning meeting during which the electrician mentioned his unspecific plan to work on the IG scrubber pump starter panel was actually a Toolbox Talk meant to discuss the work planned for that day.
The electrician apparently did not see the need for another meeting before starting his work on the LGSP cabinet. The investigation did not examine when and how Toolbox Talks were routinely held as one of the potential underlying causes of the incident.
An effective Toolbox Talk may be described as a short, job-specific meeting with relevant personnel immediately prior to commencing work, which reflects on the findings of the JHA to ensure that everyone involved is focused on achieving the task safely. Using this meeting to plan for a whole day is likely to result in personnel moving from one task to another throughout the day without another opportunity for a Toolbox Talk or similar meeting. This, in turn, would reduce the opportunities for personnel to identify any hazards which had not been systematically addressed in advance. Hazards may arise as a result of events and interactions throughout the day, which further highlights the benefits of organizing a Toolbox Talk immediately prior to starting work.
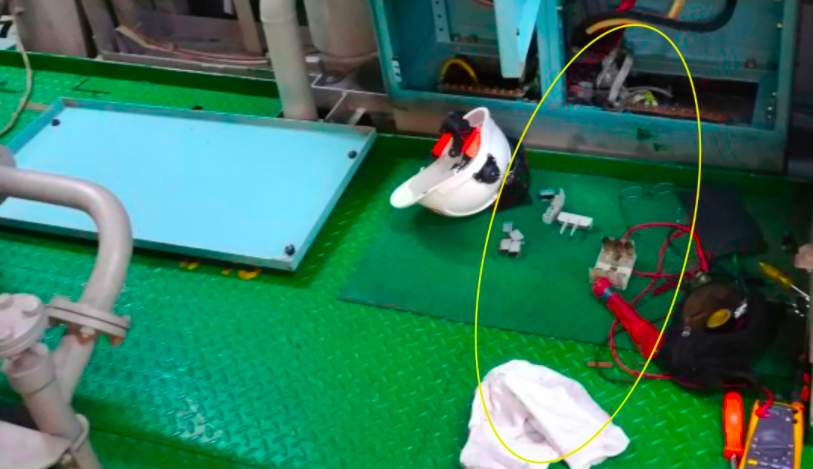
ELECTRICAL EQUIPMENT PROTECTION AND HAZARD COMMUNICATION
The investigation found that all other starter cabinets in the ship’s engine room had a physical divider between the contactor and power supply sections. The cabinet in which the electrician was working in did not have such a physical barrier. The other cabinets also had guarding installed over any exposed terminals to prevent inadvertent contact. Any of these barriers would have prevented the incident from occurring. The investigation reported that all high-voltage electrical panels installed on ships managed by the company were subsequently inspected to ensure that adequate physical barriers were in place. Furthermore, a system for preventing access to high voltage panels without proper authorisation would have provided an additional safety barrier to prevent this incident from occurring.
In addition, while the upper door had a warning sign about the 440V shock hazard, the lower panel cover had no such warning. A warning sign could have prevented the electrician from opening the cabinet without de-energizing the power. Following the incident, all high-voltage electrical panels installed on the ships managed by the company were inspected to ensure that adequate warning signs were put in place, and a sign was subsequently added to the cover of the lower panel involved in this incident.
Although the absence of the above physical safeguards was reportedly a design issue, this may be a potential example of ineffective safety control measures at both the technical and organisational level. From this perspective, a thorough verification of electrical equipment needs to be ensured, in particular with regard to quality, design and labelling. This is highlighted in the Australian Maritime Safety Authority (AMSA) bulletin “Electrical safety – an evaluation of electrical hazards” published in March 2016, which is a useful reference on the underlying issues.
RESPONSE TO ELECTROCUTION INCIDENTS
Although not contributing to the incident itself, the cadet’s well-intended response in immediately pulling the electrician away from the LGSP cabinet could have led to him also being electrocuted. When responding to a suspected electrocution incident, it is essential that the likely power source is properly isolated and that appropriate actions are taken to safely ensure that the affected individual’s body is not energised before touching it.
Hierarchy of Barrier Controls diagram
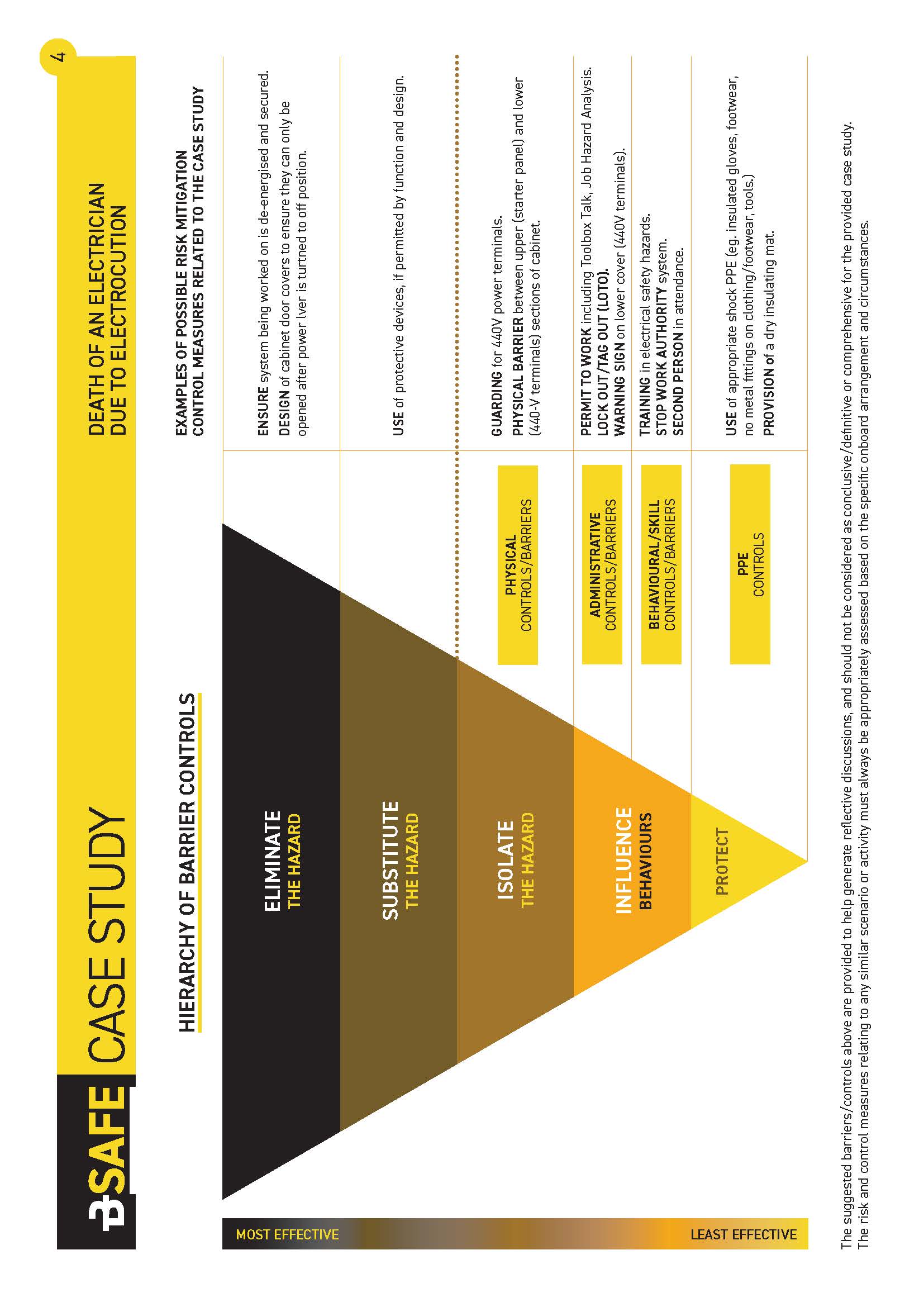
Source: Britannia P&I Club